Recently I was reading a commentary in Annals of Emergency Medicine about the problem of emergency physicians’ fatigue and associated risks for patient safety. A study of doctors in France found that 14- and particularly 24-hour shifts were associated with significant cognitive deficits, and the authors recommended that ’emergency physicians should not continue to work 24 consecutive hours’. In light of the usual gaps between work-as-imagined and work-as-done, the commentary stresses the insufficiency of these recommendations: ‘Instead of work-as-imagined solutions such as strict sleep hygiene for all physicians, we must design system mitigations that have greater potential to improve safety’ (Kellogg and Fairbanks, 2018), by being compatible with work-as-done.
“Every day people go to work and develop a work plan. This is a list, either written or in their heads, of what they hope to accomplish that day. But when people get to the end of the day, they all-too-often find that they did not accomplish everything they planned they would, and indeed their day wasn’t anything like how they’d imagined it. This distinction, between work-as-imagined (WAI) and work-as-done (WAD), is everywhere. Individuals doing their workplans are a general case of a specific cadre of people whose role it is to influence how work gets done” (Braithwaite, 2016)
‘It is impossible, in practice as well as in principle, precisely to describe how work should be done’ (Hollnagel 2017a: 11)
‘…how much humanity, how much innovation, how much dignity of daily improvisation and problem-solving goes into making even the most technologically sophisticated systems actually work’ (Dekker, 2017: 9)
An example of the difference between work-as-imagined and work-as-done is in the activity of repeat prescribing in English GP clinics.
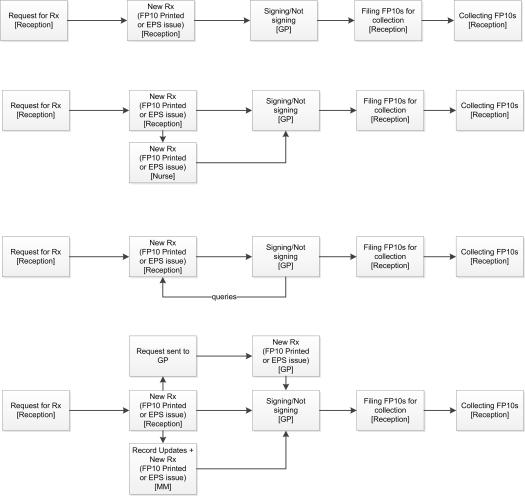
Repeat prescribing is part of the daily activities of an English general practice. A large number of patients experience this medication regime. Similarly to the ordering of drugs in hospital settings, repeat prescribing work in general practice is distributed among different roles and people, and conducted through the use of computer systems. The process involves, for each prescription, the patient (or representative), administrative staff (receptionists or clerks), sometimes a nurse, and one (or more) doctor(s). When the original prescription originates outside of the practice, when the request comes from a pharmacy, and at the time of dispensing, the boundaries of this distributed work extend beyond the surgery. The workflow-as-imagined within the clinic is simple and linear: the prescription is received by a receptionist or clerk, a new prescription for the repeat medication is printed, passed to the doctor for signing.
When we researched the activity for the evaluation of the NHS Electronic Prescription Service1, we found several variations of this workflow-as-done, especially around the many exceptions in patients’ and the variability of cases and contexts.
In terms of roles involved, these varied from receptionists only, to receptionist+nurse, receptionist(s)+dedicated clerk, and receptionist(s)+Medicine Management Team. Variations in workflow we observed in our study included in the accepted modalities for receiving patient requests (e.g. in one practice mainly over the phone), and in the agreed rules on how to deal with ‘non-routine’ repeat prescriptions (non-straightforward repeats, for example, in case of over-use, or requests for not-pre-authorised items). Thus, in case of a non-straightforward repeat, while in on place a dedicated receptionist was authorised to issue a new prescription but attach a query slip to this for the doctor to consider, in another receptionists were to submit the query to the GPs first before issuing a new prescription, and in another the GP was required to issue the prescription herself. A major peculiarity of another practice was the intermediation of a nurse between reception and GP: she dealt with and issued prescriptions with queries, while the dedicated receptionist was instructed to process ‘straightforward repeats’ only.
Overview of the repeat process in case of ‘queries’ (non straightforward repeats)
Interventions to make repeat prescribing safer would have to take into account how work is done (and why) everyday in GP practices.
By the way, within this workflow, how mindful are the doctors in signing repeat prescriptions is still an open question.
1 Lichtner V, Venters W, Hibberd R, Cornford T, Barber N. The fungibility of time in claims of efficiency: The case of making transmission of prescriptions electronic in English general practice. International Journal of Medical Informatics. 2013;82(12):1152-70.
References and some useful resources on work-as-imagined and work-as-done
Blandford, A., D. Furniss, and C. Vincent, (2014) Patient safety and interactive medical devices: Realigning work as imagined and work as done. Clin Risk, 20(5):107-110.
Dekker SWA (2017). Malicious compliance. HindSight , p8-9
Hollnagel E. (2017a) Can we ever imagine how work is done? . HindSight :10-3.
Hollnagel, E., (2017b) Why is work-as-imagined different from work-as-done?, in: R. Wears, E. Hollnagel, and J. Braithwaite (Eds). Resilient Health Care, Volume 2, CRC Press. p. 279-294.
